In-toeing and Out-toeing
Walking with the feet turned inward (in-toeing) or outward (out-toeing) often raises concerns among parents of children with these walking patterns. These are excesses of the foot progression angle (FPA). Most physician dismiss these concerns if frequent falls due to tripping are not an issue, promising that the children can be expected to outgrow these problems, or assuming that there are no functional issues or long-term consequences in terms of joint degeneration. Unfortunately, the current clinical criteria for deciding to intervene are vague. (See “More About In-toeing and Out Toeing”, below, for more details.)
How TheraTogs Can Help
For young children with FPA deviations accompanied by neuromotor disorders such as cerebral palsy, spina bifida, or cerebellar ataxia, TheraTogs Tank Top and Hipster are both needed for optimizing postural alignment and control as a foundation for improving limb use. The essential elements in achieving bone modeling to reduce excessive in-toeing will be: corrected foot joint alignment; training to gain full weight loading on the heels; and competent weight shifts onto the stance side so that the swing limb can impose more appropriate rotation forces on the stance limb.
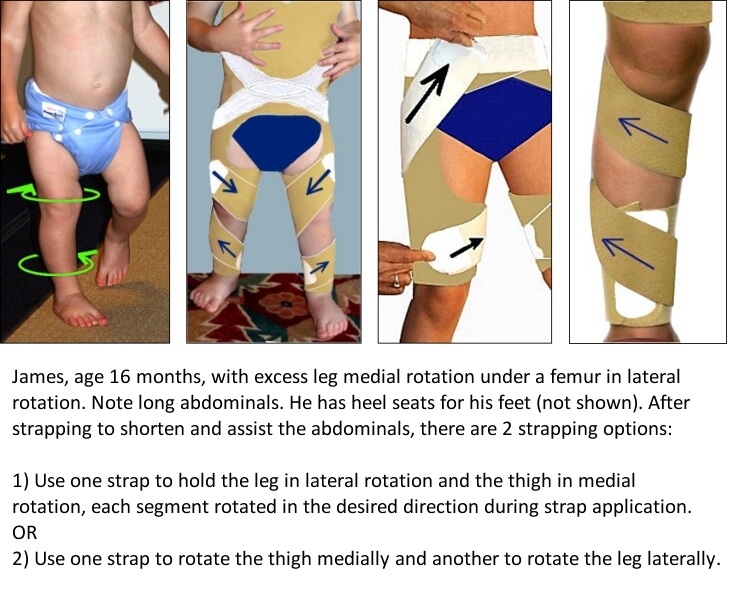
Young children with an intact CNS who exhibit in-toeing due to modeling errors in the femur and/or leg bones, or due to knee joint laxity, should be able to wear the TheraTogs Hipster only, with a TogRite strap attached to help to shorten and assist the lower abdominal muscles while the child is in training to carry his or her body weight back on the heels as well as the forefeet. With foot alignment and the lower trunk addressed, rotation straps are applied to the targeted limb segments in the direction of correction.
Using TheraTogs to reduce in-toeing and out-toeing
Movement-Related Bone and Joint Modeling – changing bone shape through the forces imposed by use history – occurs during growth. (See also physiologic adaptation.) As the pliability of growing bones and joints diminishes during childhood, so does the opportunity to influence developing bone and joint shape. Until research shows otherwise, we do not advocate attempting to correct FPA problems due to bone torsion with daily rotation strapping applications after age 6 years.
Before finding the musculoskeletal source(s) of the FPA deviation, the first step in intervening is to evaluate and address any faults in foot and ankle alignment or mobility by providing appropriate orthoses. Foot malalignments can feed FPA problems.
The potential for TheraTogs to affect growing bones by improving functioning joint alignment throughout the day is related to the maturity of the bones and to the nature of daily movement activity. TheraTogs strapping is used to gently correct functioning pelvic and limb alignment all day. Therefore, it is essential that the source(s) of deviations in FPA be identified with a careful musculoskeletal evaluation.
Contributing factors include one or more of these components: hip rotation, femoral torsion (twist), knee joint laxity allowing leg rotation, tibiofibular torsion, inward rotation of the talus inside the ankle joint, inward deviation of the long bones of the forefoot (metatarsus adductus), or outward deviation of the forefeet due to pronation (midfoot collapse).
The identification of contributing component(s) leads the clinician to form an appropriately targeted orthotic and strapping plan. In many cases, to achieve specific correction, one limb segment will be rotated into one direction while the other will be rotated into the opposite direction. For example:

Which TheraTogs Systems to Use
These TheraTogs products can support therapy goals for young children with in-toeing or out-toeing:
- Wunzi System – for infants and young preschoolers.
- Lower Extremity System – for preschoolers without CNS dysfunction
- Full Body System (FBS) – comes with limb strapping components.
Applicable Science and Therapy Approaches
Sciences that apply to the management of in-toeing or out-toeing:
- Biomechanics
- Kinesiology
- Physiologic adaptation of bone and soft tissues to use history
- Postural control
Therapy approaches that can be used to address
Movement System [Impairment Syndrome] Analysis and Management
More About In-toeing and Out-Toeing
A key element of normal bone and joint development – and related walking patterns – is the ability to manage body weight effectively. An important factor in that ability is the biomechanics of functioning bone and joint alignment. They are interconnected.
In-toeing reduces functioning foot length, encouraging a forward acceleration of the body center of mass at a time when the large immature foot is needed in front of the body to help to develop balance against falling forward while learning to walk. (Try walking with your feet turned inward. You will feel your weight carried too far forward, and will prefer to jog than walk.) A trained clinician can also find evidence of pathologic intoeing by detecting stiffness in hamstring and calf muscles – due to excessive recruitment of these muscles for balance.
“Older children (7-10 yrs) with IR [in-toeing] of the lower extremities showed a lower gait velocity, particularly in difficult balance conditions, than TD children.” [6 , p.117]
Out-toeing interferes with walking efficiency by restricting step length, imposing persistent foot pronation through the stance phase of gait, and by disabling the lever mechanism of the foot at propulsion.
As can be expected after operating daily in malalignment, long-term effects of living with excess FPA can accelerate knee joint degeneration. “Our findings show that the frontal and rotational alignment of the lower limb are aetiological factors in knee osteoarthritis.”[5, p. 209] “The more advanced the osteoarthritic stage, the greater was the reduction in external tibial torsion. Greater reduction in lateral torsion correlated with lumbar vertebral osteoporosis.”[6, p. 177]
Turner et al (1981) obtained and analyzed 1672 measurements of tibiofibular torsion using a tropometer from 836 patients in 11 diagnostic categories of knee joint pain or dysfunction. While patients with patellofemoral instability and patellofemoral chondromalacia had a significant increase in lateral tibiofibular torsion, the most important finding was a significant reduction in this torsion in patients with panarticular knee joint diseases that prompted a visit to the knee clinic.[7]
Children with “symptomatic intoeing gait” have characteristic primary and compensatory kinematic gait deviations that result in increased loading about the knee during the stance phase. In addition to problems such as frequent tripping and falling, they might complain of pain in the knee, foot, or ankle.[8]
References
- El-Shamy, Shamekh Mohamed, and Ehab Mohamed Abd El-Kafy. “Combined effect of orthotic intervention and conventional exercise training on balance and gait performance in cerebral palsy: a randomized controlled trial.” Bulletin of Faculty of Physical Therapy 27.1 (2022): 1-7.
- El-Shamy, Shamekh Mohamed, and Ehab Mohamed Abd El Kafy. “Efficacy of axial TheraTogs on gait pattern in children with dyskinetic cerebral palsy: a randomized controlled trial.” Bulletin of Faculty of Physical Therapy 26.1 (2021): 1-7.
- Mallau S, Mesure S, Viehweger E, et al. 2008.Locomotor skills and balance strategies in children with internal rotations of the lower limbs. J Orthop Res. 26(1):117-25.
- Takai S, Sakakida K, et al ( 1985) Rotational alignment of the lower limb in osteoarthritis of the knee, p. 209. Int Orthop. 9(3):209-15.
- Yagi T, Sasaki T. 1986.Tibial torsion in patients with medial-type osteoarthritic knee. Clin Orthop Relat Res. (213):177-82.
- Turner MS, Smillie IS.1981. The effect of tibial torsion of the pathology of the knee. J Bone Joint Surg Br.;63-B(3):396-8.
- Davids JR, Davis RB, Jameson LC, et al. 2014. Surgical Management of Persistent Intoeing Gait Due to Increased Internal Tibial Torsion in Children. J Pediatr Orthop. 2014 Feb 13.